

Type of pain matters
The courses are designed for bodywork professionals. They create a space to deepen knowledge, develop technique, and improve connection with the patient or client. During a session, we combine theory with intensive practice: participants watch demonstrations, work in pairs, share experiences, and discuss real cases from everyday practice. We focus on safety, conscious touch, ergonomic work, and mindfulness — so that the new skills can be applied immediately in practice.
Tension and Morning Pain
These include pain that causes stiffness and require movement to improve, as well as regional or diffuse pain that worsens after prolonged lying, sitting, or standing, and is alleviated by movement.
We also consider more intense pain that creates a sensation of heaviness or constant tension, like heavy legs, tight calves, stiff shoulders, or a rigid neck, sometimes accompanied by numbness, tingling, or muscle cramps.
Tension and Evening Pain
Tension-type pain is caused by prolonged muscle tension and tissue overload, most often resulting from repetitive activities, physical exertion, and long periods of sitting or standing. It leads to stiffness, reduced blood circulation, and dull or pressing pain. The symptoms typically build up during the day and are more noticeable in the evening.
Night pain
Nighttime pain that awakens the patient from sleep in the early pre-dawn hours, when turning from side to side, and pain in the early hours that prompts movement but isn’t significantly relieved by it.
Accute Pain
Localized, sharp, stabbing pain that inhibit movement. Movement doesn't relieve this pain.
Others
In your daily clinical practice you encounter patients with tennis elbow, golfer’s elbow, wrist pain, frozen shoulder, jumper’s knee, shin splints, hip pain, carpal tunnel syndrome, sciatica, “texting thumb,” cervical spine dysfunctions, and even breathing difficulties. Many of these musculoskeletal complaints coexist with headaches and migraines, including tension-type headaches, cluster headaches, migraines with or without aura, cervicogenic, vestibular, and ocular migraines, as well as headaches related to temporomandibular joint (TMJ) dysfunction or trigeminal nerve irritation. These seemingly different conditions are often driven by the same underlying mechanisms: repetitive overload, prolonged static postures, excessive muscle tension, and impaired tissue mobility. Understanding these shared patterns allows you to assess patients more efficiently, identify the true source of symptoms, and apply targeted, effective treatment strategies. This course provides a clinically oriented, practical framework that helps you connect the dots between peripheral musculoskeletal dysfunctions and headache presentations—so you can achieve more consistent and lasting results with your patients.
It’s important to remember that this list is not exhaustive. Symptoms never exist in isolation — they are always the result of specific mechanisms occurring in the body. That’s why diagnostics are so important: understanding where the problem comes from, rather than focusing only on what it is called.
Once you understand the principles behind our diagnostic approach, it becomes easier to deal with many other dysfunctions that are not listed here. It’s impossible to name them all — what matters most is understanding how the body reacts, compensates, and how we can support it in returning to balanceUnequal Weight Bearing: The Hidden Cause of Pain and Dysfunction
Imagine that you are bearing 5, 10, or even 15 kilograms more on one lower limb than on the other. There are several basic clinical tests that help identify the cause of this dysfunction (unequal weight bearing between the lower limbs). It is important to consider dysfunctions that may exist in:
- Muscles
- Ligaments
- Nerves
- Blocked joints
Is the two-scale test useful?
Is the two-scale test reliable?
How should it be performed correctly?
Which values should we take into consideration?First, we should reflect on the consequences of long-lasting asymmetry:
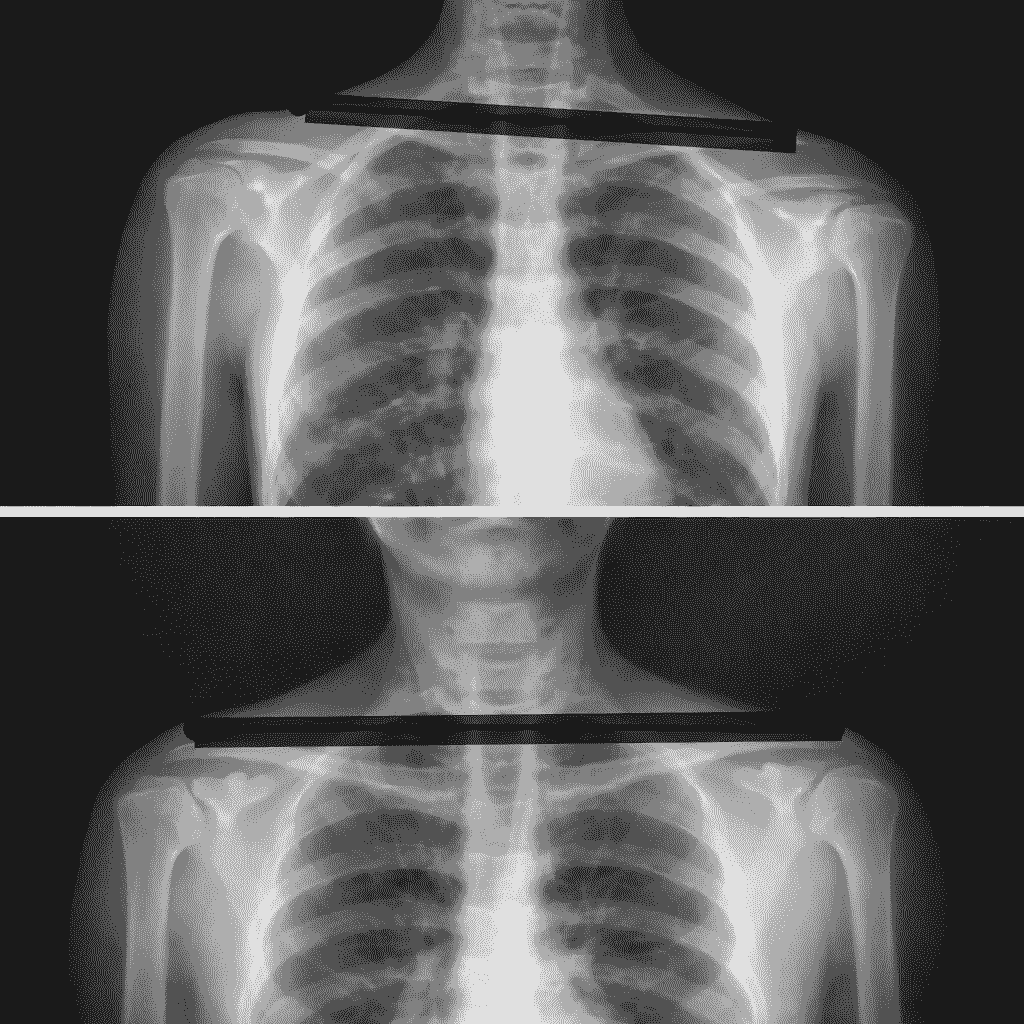
Shoulder asymmetry is not yet a true postural defect—it is rather a deviation / faulty posture. Lowering of one shoulder compared to the other may be linked to careless posture, incorrect habits, or spending too much time in a sitting position. The first symptom that should concern us is back pain and tension. Over time, joint cartilage degeneration may occur. A common cause is pelvic rotation.
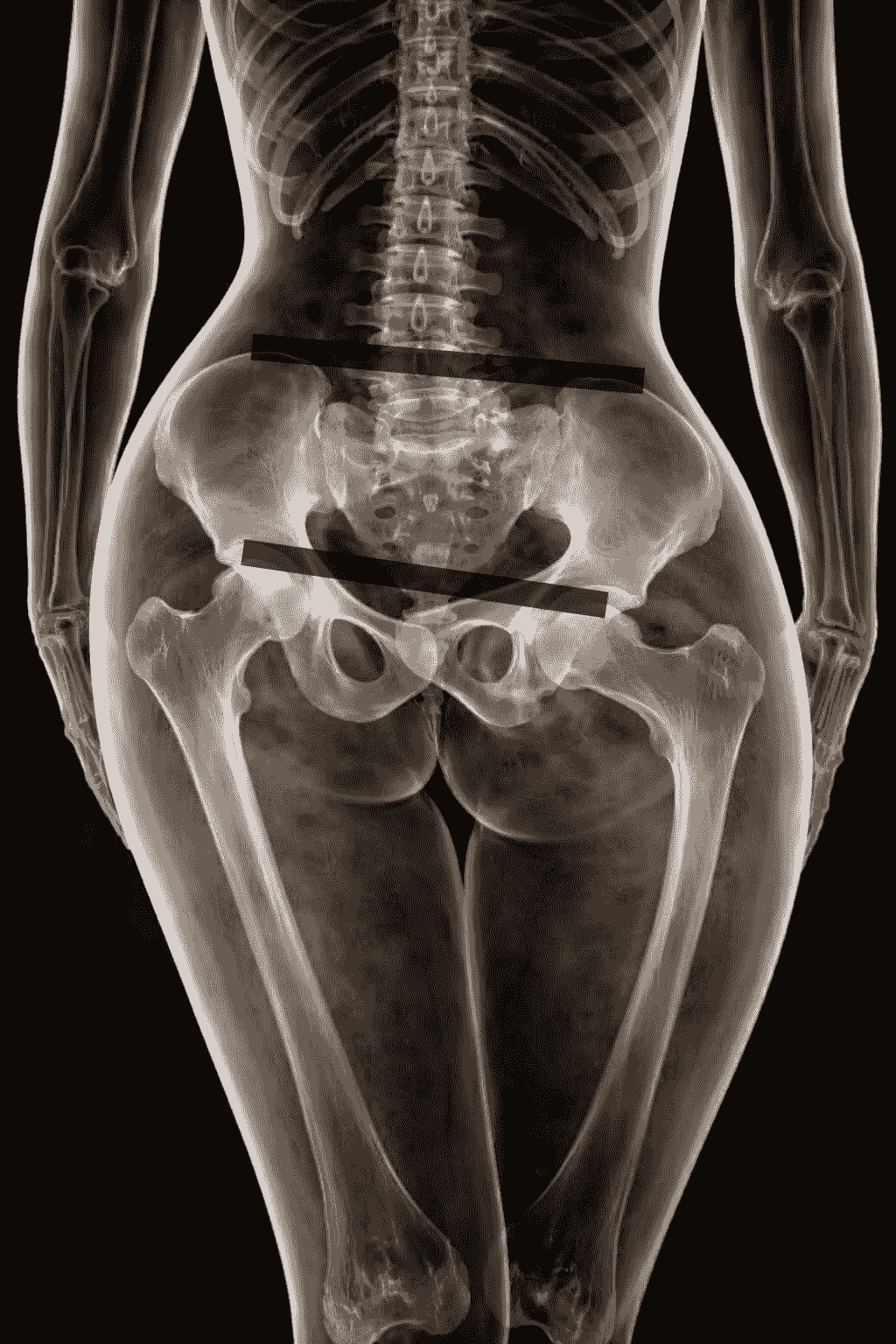
The pelvis plays a key role in spinal alignment. Due to a long-lasting incorrect pelvic position, permanent changes may develop in the lumbar, thoracic, and cervical spine. As a result, irreversible damage to intervertebral discs, facet joints, or hip and knee joints may appear, causing pain.
The pelvis is also closely related to body symmetry. It carries the entire vertebral column and has a direct connection with the lower spine and lower limbs. Because of that, any movement of the pelvis results in changes in vertebral position and affects lower-limb movement.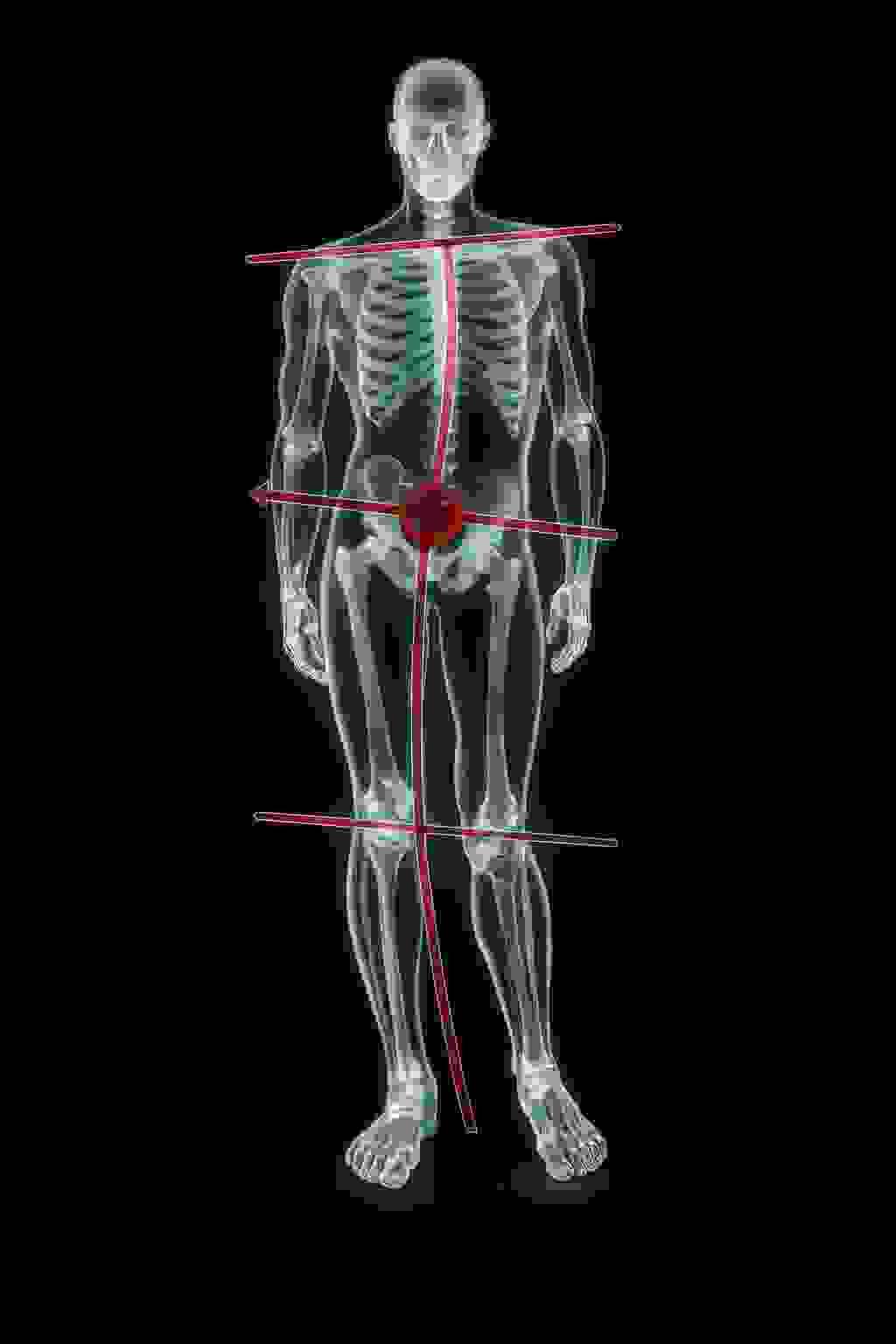
Scientists analyzing biomechanical disorders have noticed that incorrect alignment between spinal sections may lead to pathological conditions. The pelvis is the foundation of the spine, and its correct positioning strongly affects the maintenance of normal spinal curves. What happens in the pelvic girdle can also influence the cervical spine. Therefore, it is important to assess every spinal section, even if the patient complains.
In one study, the cause of vertebral fixation in over 80% of 105 patients was uneven weight bearing between the lower limbs exceeding 5 kg. After manipulation of fixed vertebrae, more than 70% of them were able to distribute weight equally while standing on two scales. Recurrence of the results after this treatment was found in 85% of patients. Better outcomes were observed when the fixed vertebrae were located in the upper cervical spine. If, during the two-scale standing test, a large difference in weight distribution between legs is detected, the craniocervical junction should be examined, including C2–C3. A difference of less than 2 kg does not seem significant.
According to Karl Lewit, a weight-bearing difference greater than 5 kg in adults and 3 kg in children should be considered pathological. However, based on my many years of clinical experience, I have concluded that even a difference exceeding 2 kg is already too large. With appropriate therapy, we are able to reduce this asymmetry to a minimum—around 2 kg, rather than 5 kg as Lewit originally suggested.
Sometimes deviations are not constant—in that case, we take average values. If the large difference is still noticeable, it should be considered significant and reassessed after treatment. It should also be verified whether the result is influenced by artefacts caused by pain in one leg.Long-term experience has shown that:
“Inconstant deviations” do not exist—only incorrect performance of the test can create them.
After 3–4 therapy sessions, values become equal (0–0) in over 90% of patients (of course, when there are no organic abnormalities, anastomosis, etc.). Equal values (0–0) can be achieved without working on the cervical spine.
What should we pay attention to?
Evaluation of head and trunk mobility:
- Forward bending
- Back bending
- Side bending
- Rotations
- Gait assessment
- Palpatory examination
Palpation should not be painful, but we cannot avoid feeling pressure. The most important factor is precise, high-quality hand work, which provides full comfort for the patient and results in relaxation of the tissues. We must pay attention to any discomfort related to the examination technique (pressure, grip). If increased tension appears because of the grip, it should be modified to minimize pain and discomfort.
A basic requirement for the diagnostic process using palpation (from a mechanical perspective) is to find the tissue that is the main source of pathology. The next step is to assess the type of tissue disorder present. It is important to identify not only the cause of the disorder, but also the factors that trigger it and maintain it.
We should remember that trigger point pain is often a result of multiple dysfunctions—one of them is unequal weight bearing between the lower limbs.
Examples in Practice

OTTAR BERG
A long-term patient, who competes in professional armwrestling, is preparing for the upcoming European Championships in Romania in just over a week. During a recent assessment using the bilateral weight distribution (two-scale test) which serves as my standard initial evaluation—he presented, for the first time since I’ve been working with him, a significant asymmetry: a 30 kg discrepancy 😮😮😮between sides.
Following the application of just one manual therapy technique, the asymmetry was reduced by 20 kg, 🤷♂️🤷♂️🤷♂️resulting in a remaining imbalance of 10 kg. While improved, this was still clinically excessive. After a second technique, the difference unfortunately increased to 15 kg—still an improvement compared to the original 30 kg. However, it wasn’t until the third intervention that complete symmetry was achieved.😀👌👌👌💪💪
This case illustrates the critical importance of assessing and restoring proper force distribution and postural balance in athletes. The two-scale test is a simple yet powerful diagnostic tool to detect and monitor such imbalances throughout the course of therapy.

RAGNAR HOLME Pt 1.
Weightlifter. Soon competition in Romania. Came with a sore back. On the two scales test, there was about 10 kg, a difference. Both sides are evenly loaded after the treatment. The pain is over. Good luck at the competition

Jack Hu
An absolute record! 🔥 Two-scale test: a 30 kg difference. One treatment—and everything was back to normal 😀. Miracles do happen 😇.
.

Martin
Over the last 2 years, this is only the second person I’ve seen with such an uneven load on the lower limbs—up to a 20 kg difference on one side 🔥 That’s a lot. After just one hanging massage, the difference dropped to only 2 kg, which is basically nothing. 👍👍👍

RAGNAR HOLME Pt 2.
Norwegian Champion. He came with a spinal shift and pain in the L-S area, left side. Therapy: 6-point pressure for 20 seconds. The pain disappeared, the spine was straight. Then a 40-minute massage. After the massage, the pain and shift returned. Finally, after pressure on 2 other points for 20 seconds, the client walked away straight and pain-free. Conclusions?










